Fluorescence-Guided Surgery
A fluorescent marker called 5-ALA makes high-grade glioma tissue glow under blue light during surgery, helping separate tumor from healthy brain.
What Is Fluorescence-Guided Surgery?
The hardest part of removing a glioma is telling where the tumor ends and healthy brain begins. High-grade gliomas do not sit in a neat capsule. Their cells spread into surrounding brain, and at the edges, tumor and normal tissue can look almost identical under the white light of an operating microscope. Standard tools like MRI and neuronavigation help plan the operation, but the brain shifts slightly once surgery begins, so a map made before the incision becomes less exact as the operation goes on.
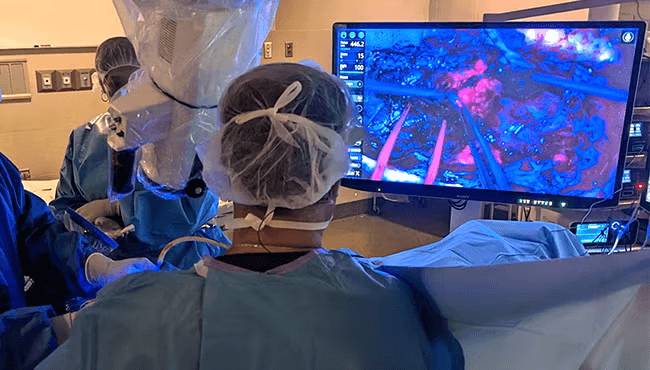
Fluorescence-guided surgery adds a way to see tumor in real time. The patient drinks a liquid called 5-aminolevulinic acid, or 5-ALA, a few hours before surgery. The brand name is Gleolan. Tumor cells take up the drug and convert it into a compound that builds up inside them. When the surgeon switches the microscope to blue light, that compound glows a pink-red color, while healthy brain stays a dull blue. The glow marks tissue that is often invisible under ordinary light.
The evidence behind this technique comes from a randomized controlled trial published in 2006, which found that surgeons using 5-ALA achieved complete removal of the contrast-enhancing tumor in about 65 percent of patients, compared with about 36 percent using white light alone, and that more patients were free of progression at six months. Those results were the basis for FDA approval in 2017 of Gleolan as an imaging aid for suspected high-grade glioma. More complete removal is associated with better outcomes, but the technique improves visualization; it is not a treatment by itself.
Dr. Sherman is a co-author of a prospective, multicenter study of 5-ALA fluorescence in high-grade glioma surgery published in the Journal of Neurosurgery in 2022, which examined how reliably the agent marks tumor across multiple academic centers. He treats high-grade gliomas and glioblastoma at Rutgers Cancer Institute in New Brunswick, NJ, the only NCI-designated comprehensive cancer center in New Jersey.
Call our office at 732-235-6333 or send us a message.
The information on this page is general educational information and is not medical advice. It does not create a doctor-patient relationship or reflect a treatment recommendation for any individual. Treatment decisions require an individual evaluation by a qualified physician.
What to Expect
Fluorescence guidance does not change the basic shape of the operation. It is a standard craniotomy with one added step before surgery and one added tool during it.
The pre-operative drink
About three hours before anesthesia, the patient drinks the 5-ALA solution mixed in water. The dose is based on body weight. From this point, the care team begins limiting bright light exposure.
Standard craniotomy under white light
The operation begins the way any brain tumor surgery does. The surgeon opens the skull, uses the operating microscope and neuronavigation, and removes tumor that is clearly identifiable under normal white light.
Switching to blue light
At points during the resection, the surgeon switches the microscope to blue light. Tumor tissue that has taken up the drug glows pink-red, while healthy brain appears blue. This helps reveal tumor at the edges that can be hard to see otherwise.
Resection guided by the glow, balanced against function
The surgeon uses the glow as one input among several. Removal is still limited by what can be taken out safely without harming areas that control speech, movement, and other essential functions. The goal remains maximal safe resection, not removal of every glowing spot regardless of risk.
Closing and pathology
The opening is closed in the usual way. Tissue removed during surgery goes to a neuropathologist for diagnosis and molecular profiling, which guides the treatment that follows.
Photosensitivity precautions
For roughly 48 hours after the drink, the patient stays out of direct sunlight and bright indoor light, because the drug temporarily makes skin and eyes more sensitive to light.
Conditions Treated with Fluorescence Guidance
Fluorescence guidance is used in surgery for gliomas, where the infiltrating edge between tumor and healthy brain is hardest to see. Each condition page covers symptoms, diagnosis, and the full range of treatment options.
Using XR Technology To Advance Medical Care
Dr. Sherman integrates VR and AR visualization into surgical planning and patient education, giving patients a clearer picture of their diagnosis and the approach to treatment.
Common Questions About Fluorescence-Guided Surgery
Before surgery, the patient drinks a medication called 5-ALA. Tumor cells absorb it and convert it into a compound that collects inside the tumor. When the surgeon shines blue light from the operating microscope, that compound gives off a pink-red glow, while healthy brain tissue stays a dull blue. The glow marks tumor that can be hard to see under ordinary white light.
Discussing Your Surgical Options
Dr. Sherman is accepting new patients at Rutgers Cancer Institute in New Brunswick, New Jersey. Whether you have just been diagnosed or you are seeking another perspective on a surgical plan, a consultation is the first step toward understanding your options.