Stereotactic Radiosurgery
Focused, high-dose radiation that treats tumors in the brain and spine precisely, without an incision, usually in a single session.
What Is Stereotactic Radiosurgery?
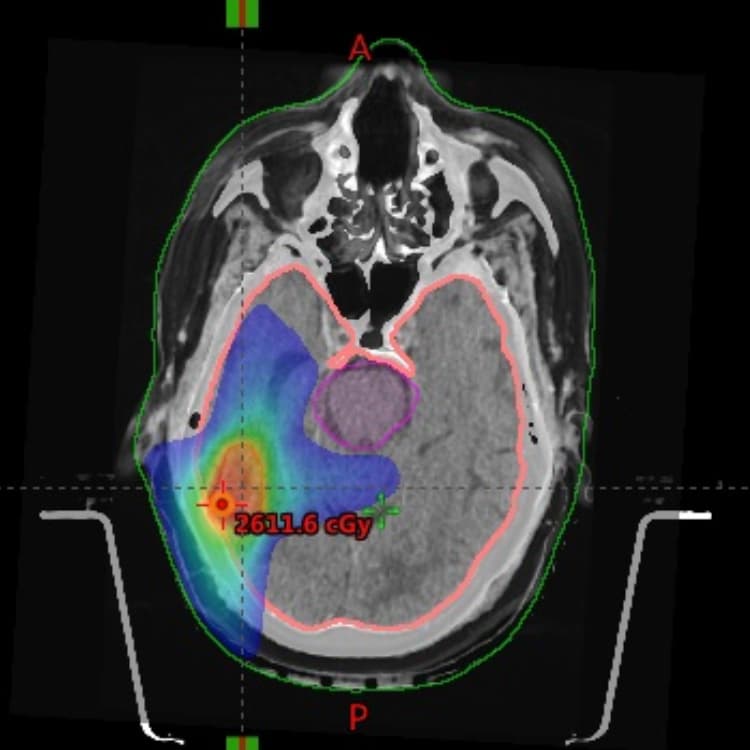
Stereotactic radiosurgery, or SRS, is a way to treat tumors with focused radiation rather than a scalpel. Despite the word surgery in the name, there is no incision, no opening in the skull, and nothing is physically removed. Many small radiation beams are aimed from different angles so they all meet at one precise point. Each beam passing through healthy tissue is weak. Where the beams converge on the tumor, the combined dose is high enough to damage the tumor cells and stop them from growing.
The radiation does not cut anything out. It alters the DNA inside the tumor cells so they lose the ability to divide and slowly die off. Because the dose drops sharply at the edge of the target, nearby healthy brain or spinal tissue receives far less radiation. This is what allows a high dose to be delivered to the tumor while limiting harm to the structures around it.
SRS is delivered by more than one specialist working together. A neurosurgeon and a radiation oncologist define the target and decide on the dose. A medical physicist and a dosimetrist build the treatment plan and confirm that the beams converge exactly where intended. The plan is checked carefully before anything is delivered, because the precision is the entire point of the approach.
Several platforms can deliver SRS. Gamma Knife uses many fixed beams of gamma rays that focus on a single point in the brain, while LINAC-based systems use a moving linear accelerator that produces X-ray beams. Rutgers Cancer Institute and Robert Wood Johnson University Hospital in New Brunswick offer Gamma Knife radiosurgery, which can be delivered with a head frame or, when appropriate, with a frameless mask-based approach.
Call our office at 732-235-6333 or send us a message.
The information on this page is general educational information and is not medical advice. It does not create a doctor-patient relationship or reflect a treatment recommendation for any individual. Treatment decisions require an individual evaluation by a qualified physician.
What to Expect
The process is built around precision, so most of the effort happens before any radiation is delivered. Here is the general sequence.
Consultation and review
A neurosurgeon and a radiation oncologist review imaging and the broader treatment plan to confirm that SRS fits the tumor and the situation. They discuss the goals, the alternatives, and the expected risks.
Planning imaging and simulation
Detailed imaging, usually MRI and sometimes CT, maps the exact size, shape, and position of the target. This imaging is used to build the treatment plan.
Immobilization
Because the target must hold still, the head is stabilized either with a lightweight frame fixed to the skull using local numbing at the pin sites, or with a custom-fitted mask molded to the face. Frames are common for single-session treatment; masks are common when treatment is spread across several sessions.
Treatment planning
The physicist and dosimetrist design how the beams will converge, set the dose, and confirm the plan protects the surrounding tissue. This step can take time, and patients often wait while it is finalized.
Treatment delivery
During delivery the patient lies still while the machine positions the beams. Nothing is felt during the radiation itself. Treatment of a single target often takes under an hour, longer when multiple lesions are treated.
After treatment
Any frame or mask is removed. Most people go home the same day, often with someone to drive them, and resume usual activities within a day or two.
Follow-up imaging
Scans are scheduled over the following months to see how the tumor responds and to watch for any changes. Imaging at roughly three and six months is common, with longer intervals after that.
Conditions Treated with Stereotactic Radiosurgery
Focused radiation is a core treatment option across several of the conditions Dr. Sherman treats. Each condition page covers symptoms, diagnosis, and the full range of treatment options.
- Brain MetastasesSRS is a standard treatment for a limited number of brain metastases, often in a single session.
- MeningiomaFocused radiation treats small, surgically risky, residual, or recurrent meningiomas.
- EpendymomaRadiosurgery can address residual or recurrent tumor after surgical removal.
- Spine MetastasesSpine-focused stereotactic radiation treats vertebral tumors while protecting the spinal cord.
Using XR Technology To Advance Medical Care
Dr. Sherman integrates VR and AR visualization into surgical planning and patient education, giving patients a clearer picture of their diagnosis and the approach to treatment.
Common Questions About Stereotactic Radiosurgery
No. Despite the name, SRS does not involve any incision, no opening in the skull, and nothing is physically removed. It uses many focused radiation beams that meet at the tumor to deliver a high, precise dose. The word surgery refers to the precision of the targeting, not to cutting. There is no wound to heal afterward.
Considering Radiosurgery or Seeking a Second Opinion?
Dr. Sherman is accepting new patients at Rutgers Cancer Institute in New Brunswick, New Jersey. Whether you are weighing stereotactic radiosurgery against surgery or looking for another perspective on a treatment plan, a consultation is the first step toward understanding your options.